Medical revenue recovery for group practices in New Jersey: a 2026 guide
Medical revenue recovery for group practices in New Jersey: how NJ multi-physician practices can recover lost revenue from denials, underpayments, and payer gaps.
Marketing Lead & Content Strategist · Jul 2026 · 9 min read
HIPAA-compliant · 13 years in NJ
Medical revenue recovery for group practices in New Jersey
Medical revenue recovery for group practices in New Jersey is the process of finding and collecting the money your practice earned but never received. For multi-physician groups across the state, that lost revenue adds up fast. HFMA estimates healthcare organizations leak 3% to 5% of net revenue annually to preventable billing failures. For a 5-physician NJ group collecting $4 million a year, that's $120,000 to $200,000 leaving the practice every 12 months, often without anyone noticing.
New Jersey group practices face a unique combination of pressure points: Horizon BCBS filing rules that changed in June 2026, NJ Medicaid (FamilyCare) renewal complexity, the federal No Surprises Act overlapping with NJ's own out-of-network protections, and a payer mix that requires credentialing across more panels than most states. Revenue recovery isn't an afterthought. For NJ groups, it's a financial survival strategy.
Key takeaways
NJ group practices lose an estimated 3–5% of net revenue annually to unbilled charges, payer underpayments, and unworked denials (HFMA).
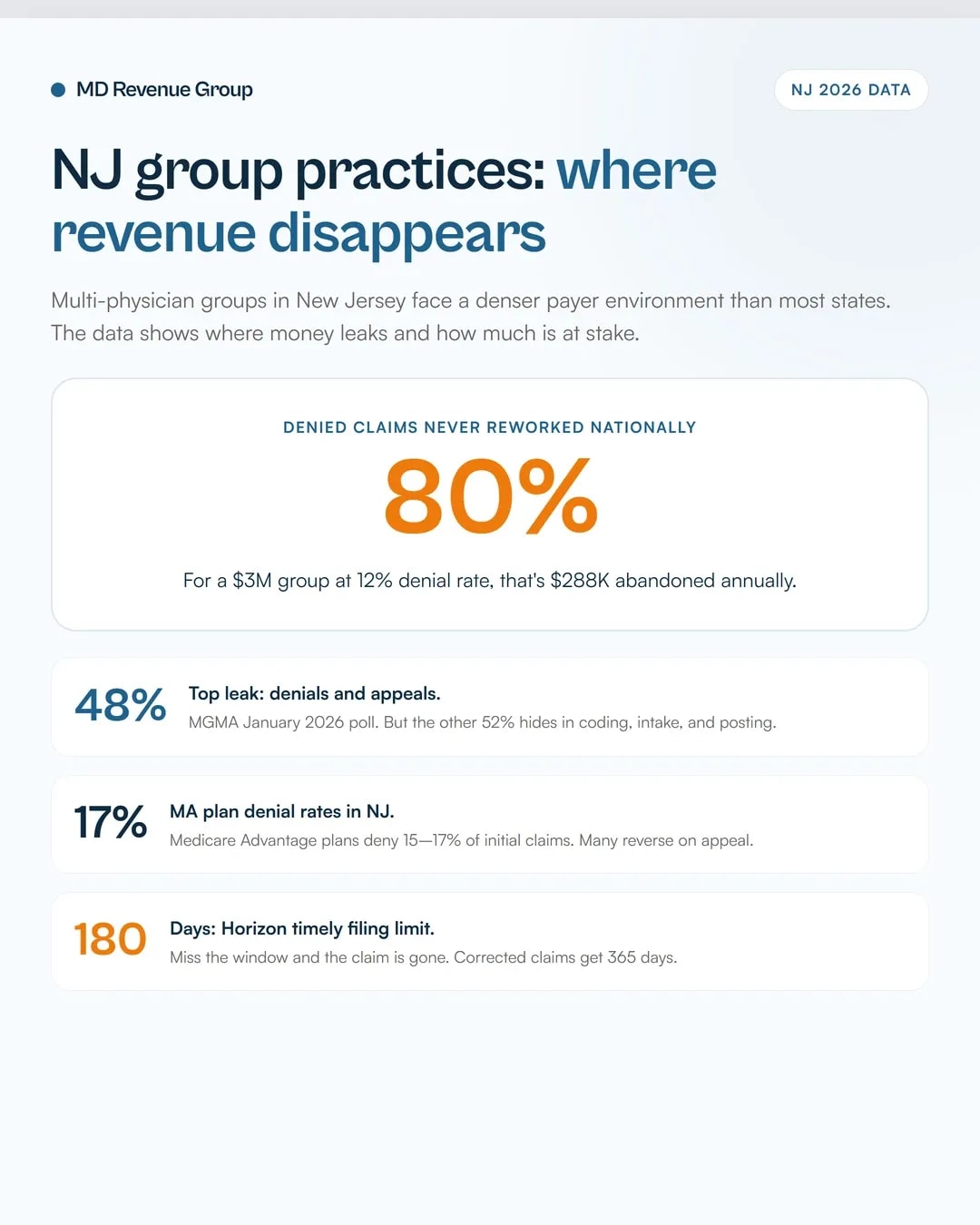
48% of medical group leaders identify denials as their top revenue leak (MGMA January 2026), but front-end errors and coding gaps account for the other half.
Horizon NJ Health stopped accepting phone disputes on June 1, 2026. All disputes must go through Availity, and practices that haven't updated their workflow are missing recovery windows.
Up to 80% of denied claims are never reworked nationally. NJ group practices handling multiple specialties and payer panels are especially exposed.
Revenue recovery is different from billing. It's the forensic review of past accounts to collect money already earned but not paid.
What medical revenue recovery actually means for NJ group practices
Revenue recovery is not the same as billing. Billing handles new claims. Revenue recovery goes backward: it audits accounts from the past 6 to 12 months to find charges that were never billed, payments that came in short, and denials that were written off without appeal.
For a group practice with 3 to 10 providers across specialties, the volume of transactions creates natural blind spots. An internal medicine provider sees 25 patients a day. A runs diagnostics that generate 4 to 6 separate CPT codes per encounter. A bills time-based codes where a 5-minute documentation gap can mean a full level downgrade. Multiply those variables across 5 providers, 20 payer contracts, and 12 months. Revenue leaks.
Recovery means pulling the data, comparing what was documented to what was billed, comparing what was billed to what was paid, and going after the difference.
Why New Jersey group practices leak more revenue than they realize
New Jersey's payer environment is denser than most states. Between Horizon BCBS (the dominant commercial carrier), Aetna, Cigna, UnitedHealthcare, and NJ Medicaid (FamilyCare), a typical group practice manages 15 to 25 active payer contracts. Each contract has its own fee schedule, modifier rules, timely filing limits, and appeal procedures.
That complexity creates leakage at every step:
Registration and eligibility errors. HFMA reports that 46% of all claim denials trace to front-end mistakes: wrong subscriber IDs, expired coverage, or missing referrals. For NJ group practices with high patient volume and multiple office locations, these errors multiply. A patient who switched from Horizon to Aetna last month shows up at your Edison office. The front desk checks the old card. The claim denies 30 days later.
Coding gaps across specialties. When a group practice includes primary care, a procedural specialty, and behavioral health under one tax ID, each specialty has different coding conventions. The biller who handles orthopedic claims fluently might underbill gastroenterology procedures by missing modifier -59 on distinct procedural services. Over a year, that pattern leaves tens of thousands on the table.
NJ's dual compliance layer. The federal No Surprises Act and NJ's own out-of-network billing protections create overlapping rules that affect how group practices bill for emergency services and out-of-network encounters. Getting it wrong doesn't just cause denials; it triggers compliance risk. Practices that haven't reconciled these two frameworks are losing revenue and taking on regulatory exposure simultaneously.
The 4 biggest revenue recovery opportunities for NJ groups
1. Unworked denials in the 90–180 day window
The industry-wide denial rate sits between 12% and 15% for initial claims (MGMA). For NJ group practices, denial rates from Medicare Advantage plans run even higher, with some MA plans denying 15% to 17% of initial claims.
The problem isn't the denial rate. It's the rework rate. Nationally, up to 80% of denied claims are never resubmitted. For a group billing $3 million annually with a 12% denial rate, that's $360,000 in denied claims. If 80% go unworked, $288,000 disappears.
Recovery means pulling every denial from the past 6 months, filtering for claims still within the payer's appeal window, and resubmitting with corrected information or supporting documentation. Most NJ commercial payers allow 90 days from the remittance advice date for appeals. Horizon NJ Health allows corrected claims within 365 days. That's a year of recoverable revenue sitting in your system.
2. Payer underpayments against contracted rates
Payers don't always pay what the contract says. Bundling edits, silent modifier adjustments, and mid-year fee schedule changes create small discrepancies ($5 to $30 per claim) that add up across thousands of claims.
A revenue recovery audit pulls EOBs for your top 20 CPT codes and compares each payment line to the contracted rate. NJ practices billing high-volume E/M codes (99213, 99214, 99215) across family medicine and pediatrics often find systematic underpayments that nobody caught because each individual shortfall looked too small to dispute.
The math changes when you count them all. 400 underpaid claims at $15 each is $6,000 per quarter. That's $24,000 a year from one CPT code at one payer.
3. Unbilled charges from documentation gaps
Providers document services they don't bill. It happens with injections, add-on codes, prolonged visit modifiers, and ancillary services that require a separate charge entry. In group practices where providers share MAs and nurses, the handoff between clinical documentation and charge capture creates gaps.
Revenue recovery cross-references chart notes against billed charges for a sample period. Any documented service that never generated a claim is recoverable revenue if it's still within the timely filing window.
This is especially common in multi-specialty NJ groups where pain management providers administer trigger point injections that don't get coded, or dermatology providers perform destructions that get lumped into the office visit rather than billed separately.
Group practices in New Jersey add and lose providers. Each provider change requires credentialing updates across every payer panel. When a new physician starts seeing patients before credentialing is complete with Horizon or Aetna, those claims process as out-of-network (or deny outright).
Revenue recovery identifies the gap period and determines which claims can be retroactively applied once credentialing is finalized. Most NJ payers will reprocess claims for the retroactive effective date if the provider's application was submitted before the date of service. But you have to ask. Payers don't volunteer that money.
NJ-specific payer rules that cause underpayments
Horizon BCBS of New Jersey
As of June 1, 2026, Horizon NJ Health no longer accepts claim disputes by phone. All disputes must go through the Availity Essentials provider portal. Practices still calling in disputes are losing recovery opportunities.
Key Horizon rules NJ groups need to know:
Timely filing: 180 calendar days from date of service for initial claims; 365 days for corrected claims
E/M bundling: Horizon applies a 50% reduction when E/M codes are billed with minor procedures. If your contract doesn't specify this reduction, it's an underpayment worth disputing.
Appeals deadline: 90 days from remittance advice date through the NJ Department of Banking and Insurance appeal form
NJ Medicaid (FamilyCare)
NJ FamilyCare renewals create eligibility gaps. When a patient's coverage lapses during the renewal period and gets reinstated retroactively, claims from the gap period often deny on the first pass. Revenue recovery means monitoring for retroactive reinstatements and resubmitting denied claims once coverage is confirmed.
Practices serving high Medicaid populations should review the NJ medical billing services page for state-specific compliance requirements.
Medicare Advantage in New Jersey
Medicare Advantage plans operating in NJ (primarily Horizon Medicare Blue, Aetna Medicare, and UnitedHealthcare Medicare Advantage) show denial rates between 15% and 17% on initial submissions. The OIG's 2026 work plan specifically targets MA prior authorization practices, and recent reports confirm that many initial MA denials are overturned on appeal.
If your group handles Medicare Advantage patients, those denials deserve a structured appeal process. The data says a significant percentage of them will reverse.
How to build a revenue recovery process for your group practice
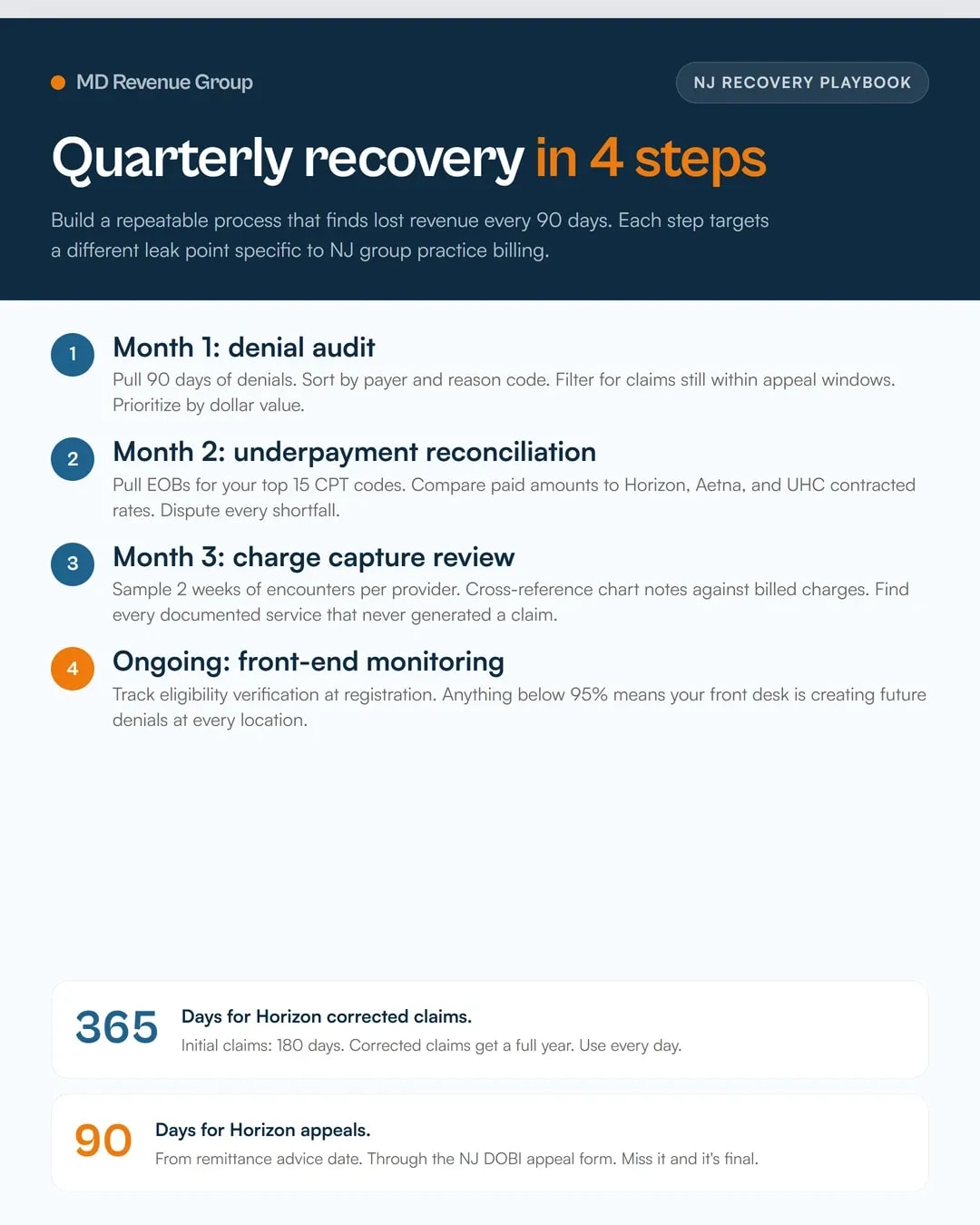
Revenue recovery works best as a quarterly discipline, not a one-time project:
Month 1: Denial audit. Pull all denials from the past 90 days. Sort by payer and denial reason. Identify which ones are still within the appeal window. Prioritize by dollar value.
Month 2: Underpayment reconciliation. Pull EOBs for your top 15 CPT codes. Compare paid amounts to contracted rates across your 3 largest payers. Flag and dispute every shortfall.
Month 3: Charge capture review. Sample 2 weeks of encounters per provider. Cross-reference clinical notes against billed charges. Identify documented services that never generated a claim.
Ongoing: Front-end monitoring. Track eligibility verification completion rates at registration. Any rate below 95% means your front desk is creating future denials. For practices managing multiple providers across NJ locations, real-time eligibility checks at every visit are non-negotiable.
When to outsource revenue recovery in New Jersey
Group practices with 3 or fewer billing staff typically don't have the bandwidth to run recovery audits while keeping current claims moving. The billing team's job is to post charges, submit claims, and work AR. Asking them to also audit 6 months of EOBs for underpayments means current collections slow down.
Outsourcing revenue recovery to a firm that specializes in NJ payer rules solves two problems: you get benchmark data (what's normal for your specialty and group size in this market) and you keep your billing team focused on today's revenue instead of yesterday's.
Many recovery firms work on contingency, meaning they collect a percentage of what they recover. If they find nothing, you pay nothing. That model aligns incentives perfectly.
For NJ group practices that also need ongoing revenue cycle management, pairing recovery with day-to-day RCM means the same team catching leaks in real time instead of finding them 6 months later.
NJ group practices don't have a revenue problem. They have a recovery problem.
If your group has 3 or more providers, bills across multiple specialties, and manages 10+ payer contracts in New Jersey, you have recoverable revenue sitting in your system right now. The question is whether you have the process to find it.
Start with your denial report. Sort by dollar value. Count how many went unworked. That number is the cost of not having a recovery process.
Or skip the self-audit and let us do it. We'll review 90 days of claims data and show you exactly where the money went.