A1712: The New NJ Itemized Billing Statement Law Every Practice Must Follow
NJ Bill A1712 requires itemized billing statements within 30 days of discharge. See what's required, the penalties, and how to prepare your practice.
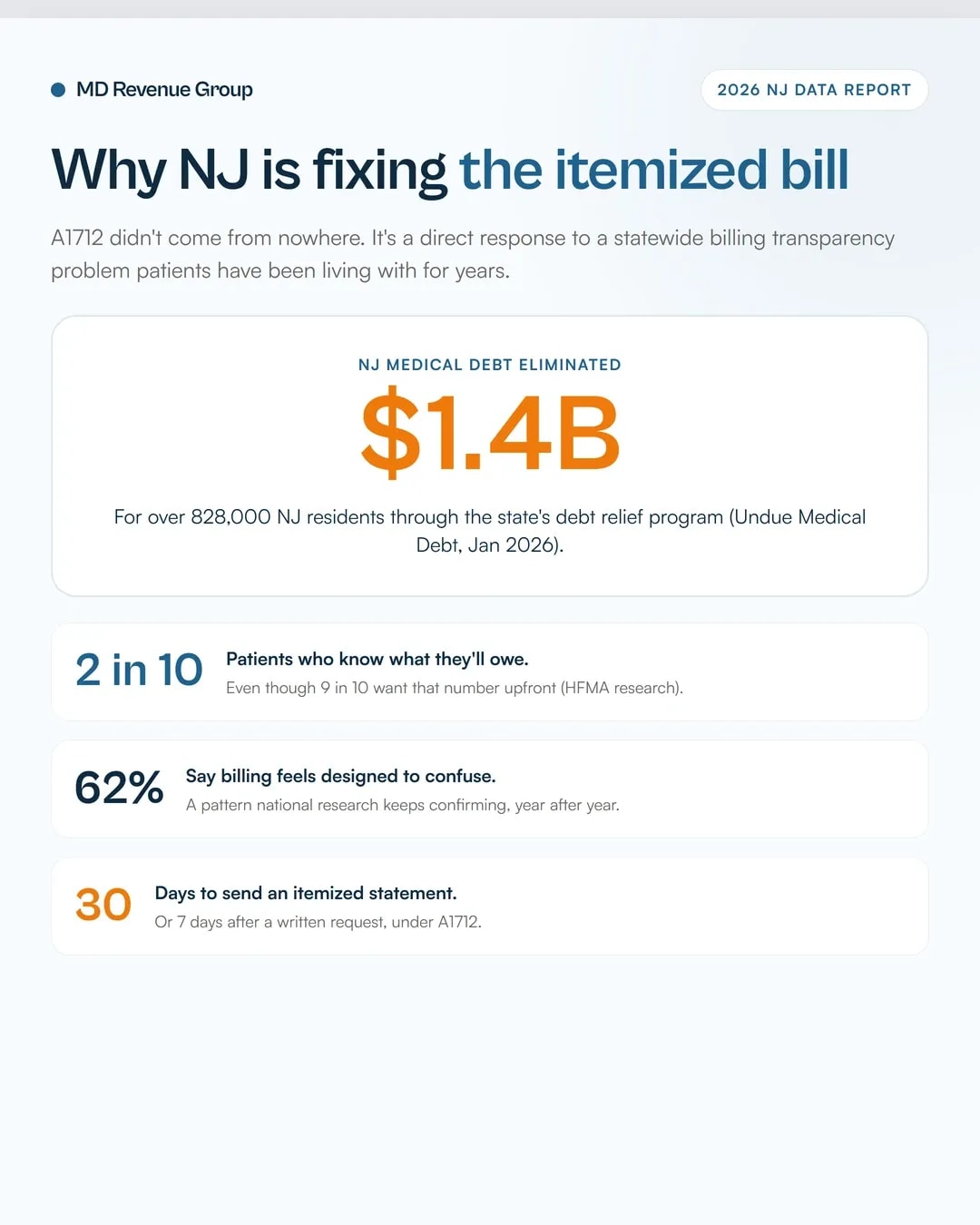
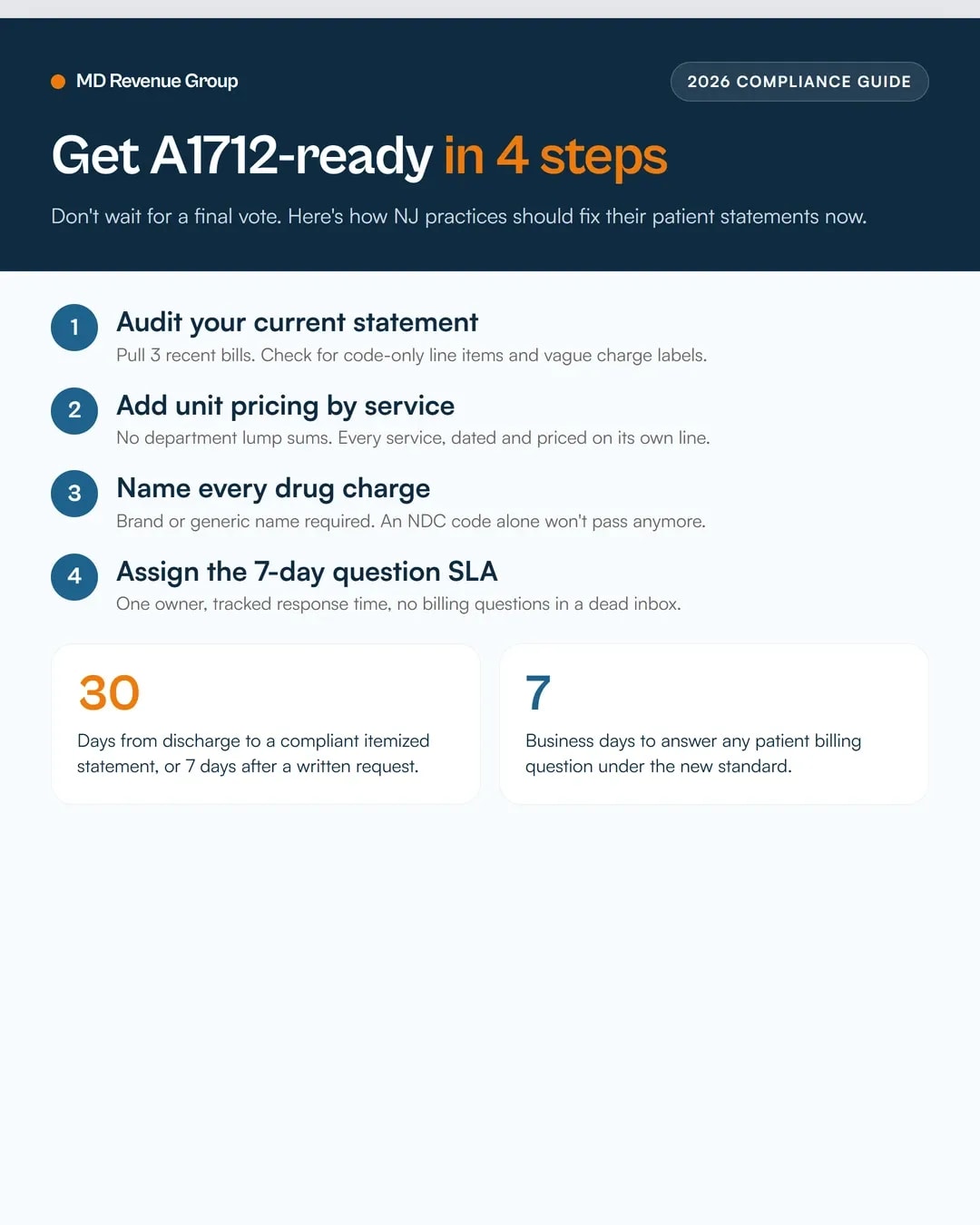
New Jersey Assembly Bill A1712 requires health care providers to send patients a consolidated, itemized statement or bill within 30 days of discharge, or within 7 days of a written request. The statement can't rely on billing codes alone or vague labels like "miscellaneous charges." It has to list each service by date and provider, show unit pricing, name drugs by brand or generic name (not just an NDC code), and mark every line as paid, billed to a payer, or owed by the patient.
A1712 picks up where its predecessor, S2795/A3860, left off in the 2024-2025 session. It was introduced January 13, 2026 and referred to the Assembly Financial Institutions and Insurance Committee. If your NJ practice or facility still generates bills from raw CPT codes and lump-sum totals, this law changes your billing workflow, not just your paperwork.
Key takeaways
- A1712 requires itemized statements within 30 days of discharge or 7 days of a written patient request.
- Bills can't use only billing codes, drug codes, or vague terms like "supply charges."
- Every line must show who's paying it: patient, insurer, or already settled.
- Facilities must answer patient billing questions within 7 business days.
- This is New Jersey's answer to a national pattern: MGMA's January 2026 poll found billing and collections issues rank among the top sources of revenue cycle leakage practices report today (MGMA Stat, Jan 2026).
What A1712 actually requires
The bill's official purpose is to establish "certain medical billing requirements concerning specific nature of charges or expenses." In practice, that means every itemized bill or statement a covered provider sends has to answer three questions clearly: what was done, what it cost, and who owes it.
You can't hide behind a CPT code and a dollar amount anymore. The statement has to describe the service in plain language an ordinary patient can understand. Technical terms are fine, as long as they're defined somewhere on the bill.
This isn't a hospital-only law in spirit, even though the bill text leans on "health care facility" language inherited from S2795. Independent practices billing patients directly for services not covered, denied, or applied to a deductible are the ones most likely to get caught flat-footed, because most EHR-generated superbills were never built for this level of detail.
A1712 is a straight re-introduction of the prior session's S2795/A3860, which cleared committee review in 2025 but didn't reach a full floor vote before the session closed. New Jersey re-files bills like this constantly, and the language rarely changes much between sessions. Treat the requirements below as close to final, not as a rough draft that might get watered down before a vote.