

CCM + RPM Concurrent Billing: The Revenue Stream Most Primary Care Practices Miss
TL;DR
- Medicare fully allows billing both Chronic Care Management and Remote Physiologic Monitoring in the same month for the same patient.
- You must track the clinical staff time for each program separately to avoid double-counting minutes and failing audits.
- Combining these codes generates over one hundred and fifty dollars per patient monthly.
- Proper documentation software with integrated timers prevents the overlapping time entries that trigger claim denials.
- Implementing this concurrent strategy funds your clinical support staff and protects your independent practice margins.
You look at your Medicare patient panel and see hundreds of patients managing diabetes and hypertension. Your clinical team spends hours on the phone adjusting medications and reviewing blood pressure logs. You bill a standard office visit when they finally come in for an appointment. You leave thousands of dollars of legitimate revenue untouched every single month.
Medicare Wants You to Bill Both
CMS created Chronic Care Management and Remote Physiologic Monitoring to keep patients out of the hospital. They know consistent monitoring costs your practice time and money. That is why they allow you to bill both programs for the same patient in the same month. Most billing departments simply do not know this rule exists.
The Rule That Changes Everything
The guidelines state clearly that you can submit claims for both CCM and RPM concurrently. You just cannot count the same minute of staff time twice. If your nurse spends twenty minutes reviewing a continuous glucose monitor, that is RPM time. If that same nurse spends another twenty minutes coordinating a referral to a nephrologist, that is CCM time.
Why Practices Leave This Money Behind
Fear drives most billing decisions in primary care. Practice managers hear the phrase concurrent billing and immediately picture an aggressive Medicare audit. They choose to bill only one code to play it safe. Playing it safe costs an average practice over six figures in lost annual revenue.
How to Beat the Fear of Audits
Auditors look for lazy documentation. They look for identical time logs copied and pasted across different billing codes. You defeat auditors by establishing clear boundaries between your monitoring tasks and your care coordination tasks. Your EHR must tell two distinct stories about the patient’s care that month.
The Golden Rule of Distinct Time
You need forty total minutes of clinical staff time to bill both base codes. CPT 99490 requires twenty minutes of care management. CPT 99457 requires twenty minutes of remote monitoring treatment management. Your staff must log these minutes in completely separate buckets within your software.
Documenting the Divide
Teach your team to label their work accurately. A note reading that the nurse spoke with the patient about their health will fail an audit instantly. A note stating the nurse spent fifteen minutes reviewing daily weight logs from a Bluetooth scale and titrating Lasix secures your RPM claim. Specificity protects your practice.
The Math Behind Concurrent Billing
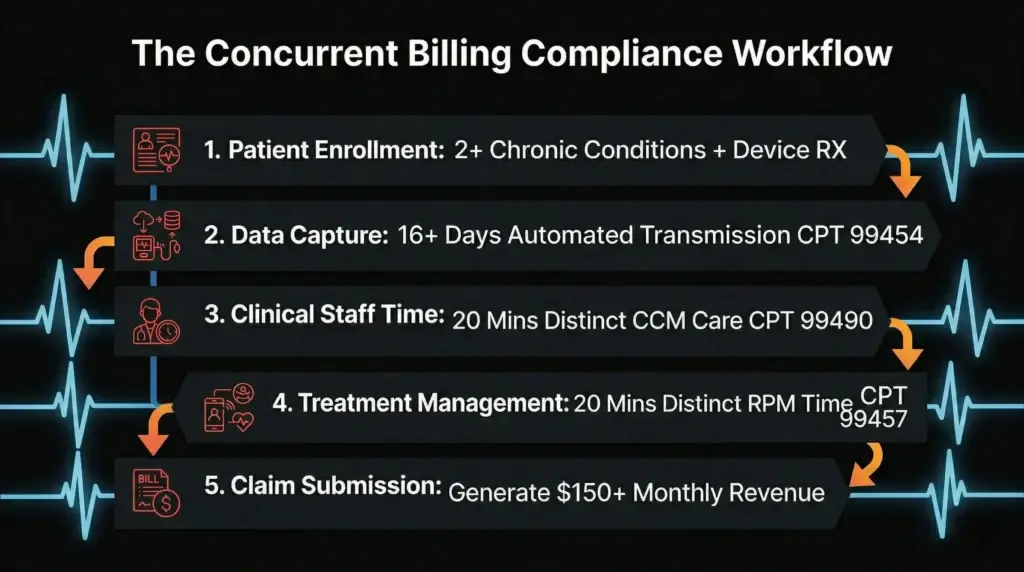
Look at the actual reimbursement rates in your Medicare fee schedule. The national average for CPT 99490 sits around sixty-two dollars per month. The base RPM code 99457 brings in another forty-eight dollars. Add the device supply code 99454, and you generate over one hundred and fifty dollars per enrolled patient monthly.
Breaking Down the CPT Codes
You must understand the specific requirements for each code to get paid. CCM requires two or more chronic conditions expected to last at least twelve months. RPM requires an FDA-defined medical device that transmits data for at least sixteen days in a thirty-day period. Meet these baseline criteria before you count a single minute of time.
Calculating the Annual Impact
Imagine enrolling just one hundred of your eligible Medicare patients into both programs. You generate an extra fifteen thousand dollars a month for work your staff is likely already doing. That totals one hundred and eighty thousand dollars in new annual revenue. That covers the salary of two full-time medical assistants.
Setting Up the Workflows
Good intentions do not process claims. You need a mechanical workflow that captures every minute of staff effort without disrupting patient care. The front desk, the medical assistants, and the providers must all know exactly what to do. Confusion in the clinic leads to missing codes in the billing department.
Identifying the Right Patients
Start with your most complex cases. Run a report in your EHR for Medicare patients with both diabetes and heart failure. These patients already require intense monitoring and frequent care coordination. They are the perfect candidates to pilot your new concurrent billing program.
Choosing the Right Devices
Do not force patients to manually log their vitals. You will never meet the sixteen-day requirement for CPT 99454. Ship cellular-connected blood pressure cuffs and scales directly to their homes. The devices transmit data automatically to your portal the moment the patient steps on the scale.
The Technical Requirements of the Devices
CMS strictly regulates what counts as a medical device for RPM. You cannot tell a patient to buy a smartwatch and start billing Medicare for the data. The equipment must meet the FDA definition of a medical device. It must also automatically transmit the physiologic data without manual patient intervention.
Avoiding the Manual Entry Trap
Some vendors sell cheap devices that require patients to type their readings into a smartphone app. Medicare explicitly prohibits billing CPT 99454 for patient-reported data. If an auditor discovers your patients type their own blood pressure numbers, they will claw back every cent you collected. Always insist on cellular or direct Bluetooth transmission.
Managing Device Inventory
You also need a reliable system for tracking who has which device. If a patient stops transmitting data, you must retrieve the expensive equipment and reassign it. Lost devices destroy the profit margins of your monitoring program. Treat your device inventory with the same strict controls you apply to your vaccine refrigerators.
Training Your Clinical Team
Your medical assistants will make or break this program. They do the bulk of the work required to bill these codes. If they view time tracking as an administrative burden, they will forget to do it. You must show them how this revenue directly supports their jobs and the clinic’s resources.
Shifting the Staff Mindset
Stop treating billing as a dirty word in the clinical space. Explain to your nurses that capturing this revenue allows the practice to hire more help. Show them the direct link between proper documentation and a lighter daily workload. A fully funded care management department runs much smoother than an underfunded one.
Automating the Time Tracking
Never rely on sticky notes or manual spreadsheets to track clinical minutes. Use care management software that features an integrated timer. The nurse clicks a button when she opens the patient’s chart and clicks it again when she finishes the task. The system automatically categorizes the time for the billing team.
Overcoming the Patient Pushback
Patients will ask questions when they see new charges on their Medicare summary notices. Some will call the office angry about unexpected bills. You must prepare your front desk to handle these calls with confidence and clarity. The conversation starts long before the first claim goes out.
Selling the Care Plan
Frame the program as a premium service. Tell the patient they now have a dedicated nurse watching their vitals every single week. Explain that this program prevents emergency room visits and keeps them living independently at home. When patients understand the value, they rarely complain about the service.
Managing the Copay Conversation
Medicare Part B covers both programs, but the standard twenty percent coinsurance usually applies. Be honest about this upfront. Most patients have secondary or supplemental insurance that covers this gap entirely. For those who do not, explain that a ten-dollar monthly copay is far cheaper than a hospital admission.
When Claims Get Denied Anyway
You will face initial denials when you start billing concurrently. Medicare administrative contractors sometimes have outdated automatic edits in their systems. Do not let a few initial rejections scare you away from the program. You just need to know how to push back and win the appeal.
Spotting the Common Mistakes
Check your diagnosis codes first. A claim for CCM will fail if you only list one chronic condition on the claim form. Ensure your RPM claim points to a diagnosis that justifies the specific device you prescribed. A glucometer paired with a diagnosis of osteoarthritis will trigger an immediate denial.
Fixing Clearinghouse Glitches
Sometimes your clearinghouse strips necessary modifiers before the claim even reaches Medicare. Review the raw electronic data interchange files if you see a pattern of unexplained rejections. Work with your vendor to ensure the claims transmit exactly as your billers coded them. A simple mapping error can freeze your entire revenue stream.
Auditing Your Own Practice
Never wait for Medicare to tell you that your billing practices are flawed. You must proactively search your own records for mistakes. Pick ten charts every quarter and review the care management logs line by line. You will find the errors before they become a systemic liability.
What to Look For
Check the timestamps on the nursing notes. If you see RPM time logged from two o’clock to two-twenty, and CCM time logged from two-fifteen to two-thirty-five, you have an overlap. That five-minute overlap invalidates the distinct time requirement. You must train your staff to close one task completely before opening the next.
Correcting the Course
When you find these errors during an internal audit, do not panic. Use them as training opportunities for your clinical staff. Show the nurse exactly where the times overlapped and explain how to fix it next time. Constant, gentle correction builds a culture of extreme accuracy within your clinic.
The Cost of Doing Nothing
Primary care margins grow thinner every year. Overhead costs rise while standard evaluation and management reimbursement rates stagnate or drop. You cannot run a profitable practice simply by seeing more patients for shorter visits. You must find ways to get paid for the work happening between those visits.
Watching Margins Shrink
Every time a nurse spends thirty minutes coordinating a hospital discharge without billing for it, your practice loses money. You pay the nurse’s hourly rate while generating zero revenue to cover it. This invisible bleed slowly drains the financial life out of independent medical practices.
The Better Alternative
Concurrent billing fixes this exact problem. It converts your biggest expense, which is clinical staff time, into a predictable monthly revenue engine. It rewards your practice for providing excellent, proactive medical care. You just have to build the courage and the systems to claim it.
Building a Sustainable Future
You do not have to figure this out alone. The rules change constantly, and keeping up with CMS updates is a full-time job. Bringing in experts allows you to focus on clinical care while someone else handles the compliance. You need a partner who understands the deep mechanics of Medicare billing.
The Role of Expert Guidance
A specialized billing team audits your workflows before a single claim drops. They review your documentation templates and train your staff on exactly what to write. They catch the overlapping time entries that would otherwise trigger a catastrophic audit. Professional oversight turns a risky venture into a secure financial asset.
Making the Transition
Start small. Pick fifty patients and run the program for three months. Watch the claims process and measure the actual revenue hitting your bank account. Once you see the math work, scale the program across your entire eligible patient panel and watch your practice thrive.
Your Next Move
The money is sitting there waiting for you to claim it. Your staff is already doing the hard work of managing these complex patients. Stop giving that time away for free. Start building the documentation habits that will protect your practice and secure your financial future.
If your practice is struggling with concurrent billing rules, MD Revenue Group can help. Based in Jersey City, NJ, we work with providers across the country to capture missed revenue and build clean RCM workflows. Reach out to our team for a free consultation to review your current processes. We would love to learn about your practice and see what is possible.