
Behavioral Health Integration Billing: New CMS Codes That Most Practices Aren’t Using
TL;DR
- CMS has reimbursed behavioral health integration billing services since 2018, but most primary care practices still aren’t billing for them, leaving recurring monthly revenue uncollected.
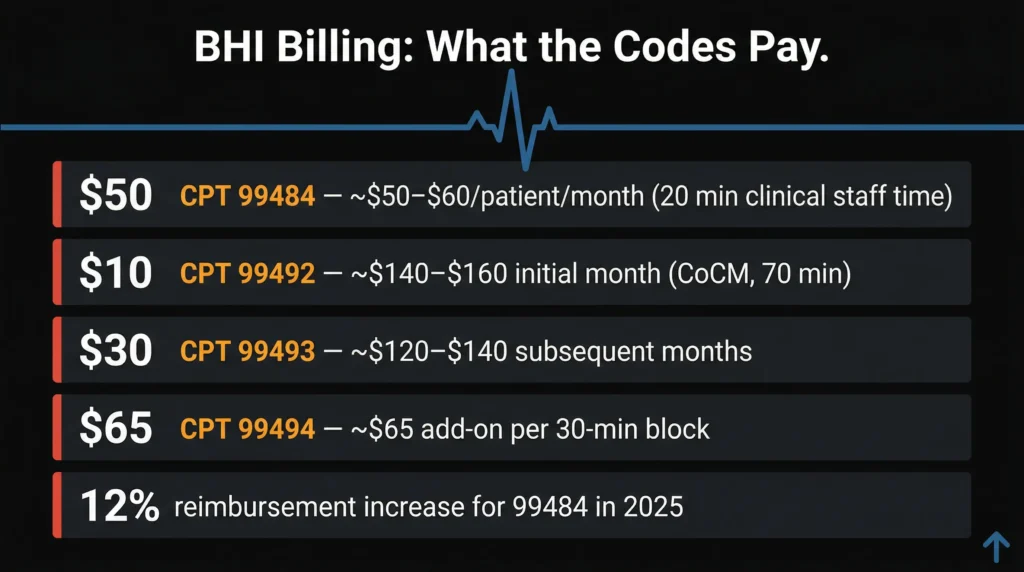
- The core codes are CPT 99484 (General BHI) and CPT 99492/99493/99494 (Psychiatric Collaborative Care), each with distinct requirements and reimbursement rates.
- You only need 20 minutes of clinical staff time per patient per month to bill CPT 99484 — the physician does not need to do all the work.
- In 2025, CMS raised reimbursement for 99484 by roughly 12% and opened BHI billing to Rural Health Clinics and FQHCs for the first time.
- BHI can be billed alongside Chronic Care Management (CCM), creating two separate recurring revenue streams from the same patient panel.
More than one in five American adults lives with a mental, behavioral, or psychiatric health condition. Odds are, a significant portion of your patient panel is already in that group. CMS has been reimbursing Behavioral Health Integration services since 2018, and most practices still haven’t touched the codes.
That’s not a clinical failure. It’s a billing knowledge gap, and it’s costing practices thousands of dollars every single month.
What BHI Actually Is (and Why CMS Is Paying for It)
Behavioral Health Integration Billing means bringing mental and behavioral health care into the primary care setting, rather than sending patients to navigate a completely separate system. For patients with depression, anxiety, or substance use disorders, this kind of integrated care improves outcomes, increases treatment adherence, and reduces total cost of care. CMS formalized reimbursement for BHI because the data supports it: the Psychiatric Collaborative Care Model alone has been shown to generate up to $6.50 in savings for every dollar spent on it.
For your practice, this means you’re likely already delivering care that qualifies for reimbursement. The question is whether you’re capturing it on the claim.
The Two BHI Tracks: General BHI vs. Collaborative Care
General BHI (CPT 99484) is the lower-barrier entry point. It requires 20 minutes of clinical staff time per patient per month, covering assessments with validated rating scales, care plan work, behavioral health monitoring, and provider coordination. A nurse, licensed social worker, or other qualified clinical staff member can deliver most of it under the billing practitioner’s direction. Reimbursement runs approximately $50 to $60 per patient per month, billed once per calendar month.
Psychiatric Collaborative Care Management (CoCM) is the more structured tier, built for complex patients who need a full team. CPT 99492 covers the first 70 minutes in the initial month at around $140 to $160. CPT 99493 covers subsequent months at roughly $120 to $140. CPT 99494 is a 30-minute add-on unit at approximately $65. This model requires three distinct roles: the billing practitioner, a trained behavioral health care manager, and a psychiatric consultant. One hard rule: you cannot bill both General BHI and CoCM for the same patient in the same month.
What Changed in 2025 and Why Now Is the Right Time
CMS increased reimbursement for CPT 99484 by approximately 12% in 2025. For a practice with 50 eligible patients billed every month, that’s a meaningful boost to predictable recurring revenue without adding new services. CMS also allowed Rural Health Clinics and Federally Qualified Health Centers to bill individual BHI CPT codes directly for the first time, after the bundled G0511 workaround expired on July 1, 2025.
On top of that, CMS expanded the eligible workforce for CoCM, formally recognizing licensed professional counselors and marriage and family therapists as qualified behavioral health care managers. If your practice previously lacked the staffing to run a CoCM program, that barrier is lower now than it has ever been.
The Documentation Setup You Need Before Billing Anything
Every BHI patient needs an initiating visit first: a face-to-face encounter where you complete an initial assessment and obtain written consent. That consent must cover three things — that cost-sharing applies, that only one practitioner can bill BHI per month, and that the patient can stop services at any time. Skip this step and every claim that follows is at risk.
Once services begin, monthly billing requires documented time from the right people. For General BHI, the qualifying minutes come from clinical staff, not the physician. For CoCM, they come from the behavioral health care manager. Use validated scales like the PHQ-9 or GAD-7 to demonstrate systematic monitoring. “Discussed behavioral health” in a progress note is not documentation. A PHQ-9 score with a dated care plan update is.
The Hidden Revenue Play: Stacking BHI With CCM
Behavioral Health Integration Billing can run concurrently with Chronic Care Management for the same patient in the same month. They are separate programs with separate time requirements, and CMS allows both to be billed together. Many patients who qualify for BHI also carry chronic physical diagnoses — diabetes, hypertension, COPD — making them eligible for CCM as well. Billing only one means leaving the other uncollected.
The rule to follow: time documented for BHI cannot double-count toward CCM. Track each program’s minutes independently in the medical record. Done correctly, this creates two separate monthly recurring revenue streams from a patient population you’re already managing.
Why Most Practices Still Haven’t Started Behavioral Health Integration Billing
The most common assumption is that you need to hire a dedicated behavioral health professional before you can bill BHI. That’s not true for General BHI. A nurse or licensed clinical social worker already on your team can deliver the qualifying services under your supervision, with no new hire required. The staffing barrier is mostly a myth.
The real barrier is workflow visibility. BHI codes don’t surface automatically in most EHR billing prompts. Unless someone on your team is specifically trained to identify and code these services, they simply don’t get submitted. That’s a recurring monthly miss for every eligible patient in your panel, compounding quietly over time.
How MD Revenue Group Helps You Capture BHI Revenue
Getting BHI billing right the first time requires more than knowing the codes. It means building consent workflows, staff training, documentation templates, and claim submission processes that work together without adding friction to your providers’ day.
MD Revenue Group works with primary care and specialty practices across the country to set up BHI billing programs from the ground up. Based in Jersey City, NJ, our team handles the coding, the compliance checks, and the claim follow-up so your staff can stay focused on patients. If you have Medicare patients with behavioral health conditions and you’re not billing BHI yet, reach out for a free consultation. Let’s find out exactly how much revenue your practice has been leaving behind.