
What NJ Doctors Need to Know About AI and Medical Billing
TL;DR
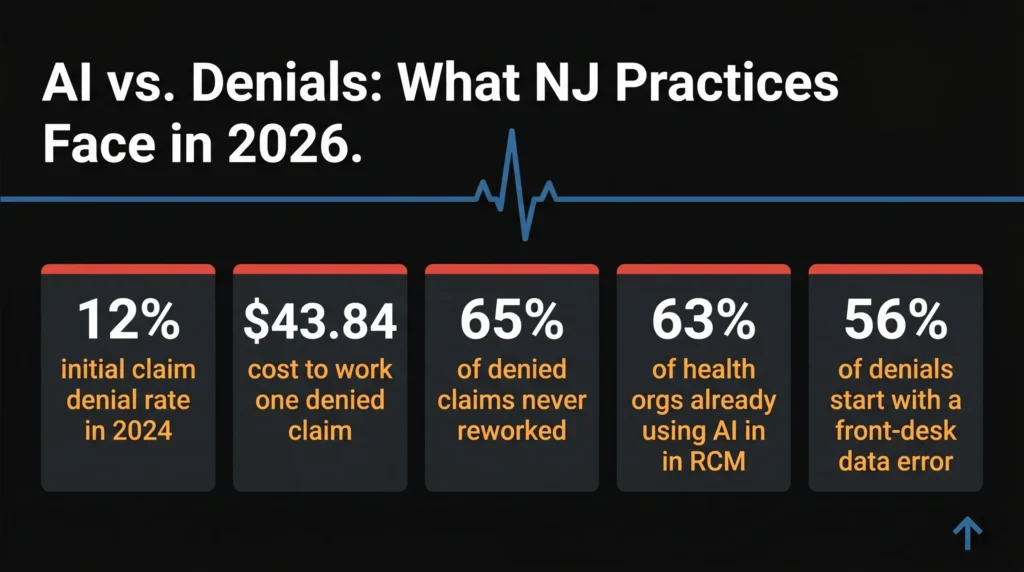
- Claim denial rates hit nearly 12% in 2026 and are still climbing – AI is the only tool catching up to payer algorithms.
- 63% of healthcare organizations are already using AI for revenue cycle work. Most NJ practices aren’t yet.
- AI works best upstream: eligibility checks, claim scrubbing, and denial prediction before submission.
- “AI-powered” is a marketing label. Ask vendors for proof, not pitch decks.
- You don’t need to rebuild your entire billing operation. Start with your top 5 denial reasons and work backwards.
A New Jersey cardiologist spent 14 months chasing $212,000 in denied claims.
His billing team was experienced. His coders knew their CPT codes. His front desk ran eligibility checks every morning.
And still, every month, the same payers kept denying the same claim types. Slightly different reason codes. Slightly different documentation requests. The goalposts moved just enough to keep the denials coming.
What he didn’t know: the payers had already deployed AI to find those reasons faster than his team could manually prevent them.
That’s the fight in 2026.
The math stopped working for manual billing
41% of healthcare providers now report that more than 1 in 10 of their claims is denied. Three years ago, that number was 30%.
It keeps going up.
Up to 65% of those denied claims are never reworked. That revenue is simply written off.
For a busy NJ internal medicine practice billing 400 claims a month, that’s not a billing problem. That’s a slow leak in your business.
Working a single denied claim – investigating the reason, correcting the problem, resubmitting, following up – costs an average of $43.84 in administrative labor. Multiply that across a year and you’re looking at a six-figure line item that doesn’t show up anywhere on your P&L.
Your billing team isn’t failing. The game changed.
By 2026, insurance payers are using their own AI to find reasons to deny claims. They have years of claims data. They have machine learning tuned to their own policy fine print. And they’re running it on every single claim you send.
Manual billing versus payer AI is not a fair fight.
What AI in billing actually does (and doesn’t do)
Before any NJ practice buys into the AI pitch, here’s what the technology actually looks like on the ground.
AI is most valuable when it supports three layers of work: front-end readiness (insurance verification, prior authorization, documentation checks), claims accuracy (CPT and ICD-10 alignment, charge validation), and back-end recovery (denial prioritization, root-cause analysis, payer-specific next steps).
The biggest wins come at the front end.
The most preventable denials aren’t driven by complex payer disputes. They start with data errors at patient registration. Wrong insurance ID. Outdated group number. A policy that lapsed two weeks ago. AI catches those before the claim ever leaves your practice.
That’s the shift that matters: from reacting to denials to preventing them.
Predictive analytics can score claims for denial risk before submission, routing high-risk claims for human review. That presubmission checkpoint is where the clearest time savings are realized in independent practice settings.
But here’s what AI can’t do.
AI doesn’t eliminate denials entirely. Errors tied to payer-specific policy changes, incomplete clinical documentation, or gaps in office workflow still require human oversight. Any vendor telling you otherwise is selling you something that doesn’t exist yet.
Fully autonomous billing remains a marketing phrase more than an operational standard in 2026.
The practices winning right now aren’t the ones who automated everything. They’re the ones who put AI in the right spots and kept skilled people where judgment actually matters.
What this means for NJ practices specifically
New Jersey practices carry a specific burden that practices in less regulated states don’t.
You’re dealing with some of the highest Medicare Advantage penetration rates in the country. NJ’s payer mix skews toward commercial insurers with complex, plan-specific rules. And your denial rates on prior authorizations run above the national average.
Current challenges include higher Medicare Advantage denial rates, stricter enforcement of prior authorization following regulatory changes, and persistent revenue cycle staffing gaps.
On top of that, NJ practices compete for billing talent in a tight labor market. Experienced RCM staff are expensive and hard to keep. When someone leaves, institutional knowledge walks out with them.
AI doesn’t replace that knowledge. But it does stop your revenue cycle from being held hostage to it.
56% of providers say patient information errors are a primary cause of claim denials. That’s a front-desk problem. And it’s completely fixable with the right eligibility verification tools running in the background before each appointment.
Small NJ practices, the solo internist in Hoboken, the two-physician family practice in Montclair, aren’t going to buy enterprise RCM platforms. But they can access the same AI capabilities through an outsourced billing partner who’s already built that infrastructure.
That’s worth understanding before you assume AI is only for big health systems.
How to evaluate AI claims without getting sold smoke
Every billing software vendor in 2026 has “AI-powered” somewhere in their marketing.
Most of it is rebranded rule-based automation. The rules don’t learn. They don’t adapt to your payer mix or your specialty. They just run the same checks they ran in 2021 with a new label on the box.
The test is simple: ask any vendor to take a denied claim from your last quarter and walk through exactly how their AI would have prevented it. Platforms doing real work answer that question directly. Platforms running rebranded automation change the subject.
Ask for named client case studies, not aggregate statistics. Ask what their first-pass clean claim rate is for practices in your specialty. Ask how their system handles payer policy updates – do they push rule changes manually, or does the model adapt?
Half of healthcare leaders cite data privacy and security concerns as the biggest barrier to AI adoption. That concern is legitimate. Any AI system touching your claims data needs to be HIPAA-compliant, with documented security protocols and a Business Associate Agreement in place.
If a vendor is vague on any of that, walk away.
Three things you can do right now
You don’t need to overhaul your entire revenue cycle this month. Here’s where to start.
Pull your denial data. Look at your last 90 days of denials and find the top 5 reason codes. Those five codes tell you exactly where your process is bleeding. Everything else comes after.
Check your eligibility workflow. Nearly 8 in 10 providers still rely on multiple disconnected solutions to collect the information needed for a single claim submission. If your front desk is manually checking eligibility on a payer portal the morning of the appointment, you’re one typo away from a denial. Real-time automated eligibility checks aren’t expensive. They’re just not standard yet.
Ask your billing partner the hard question. Whether you bill in-house or outsource, ask: what percentage of our claims are denied on first submission? What’s our clean claim rate? If you don’t know those numbers, you can’t improve them.
The practices seeing the strongest results use AI to surface patterns and reduce manual repetition, while keeping skilled billing staff responsible for decisions that require clinical context, payer-specific knowledge, and professional accountability.
That’s not a technology strategy. That’s just running a tight operation.
The payers already made their move
The cardiologist from the beginning of this article eventually found the pattern in his denials. Same three CPT codes. Same two payers. A modifier rule that had quietly changed eight months earlier.
Once he knew that, the fix took two days.
The problem was the eight months it took to find it.
AI finds that pattern in the first week. Before the denials stack up. Before the rework buries your billing staff. Before $212,000 disappears into write-offs.
NJ practices that adopt the right tools in 2026 won’t just collect more revenue. They’ll stop losing the revenue they already earned.
Work with a billing team that’s already there
If your practice is losing revenue to denials, eligibility gaps, or an aging AR, MD Revenue Group can help.
Based in Jersey City, NJ, we work with practices across New Jersey and nationwide to run cleaner revenue cycles – with the tools, the expertise, and the accountability to back it up. Reach out to our team for a free billing consultation. We’d love to take a look at your numbers and tell you exactly where we can make a difference.